How to prevent a perineal tear during childbirth
Perineal trauma/ pelvic floor tearing: It’s an ever evolving fear amongst women I treat (especially first time mums - me included!). As always, knowledge is power and sticking your head in the sand “hoping” this won’t happen to you unfortunately isn’t a great strategy!
Counselling women prior to delivery and treating women after perineal tears is something I do everyday. There is SO much I would like to write here. This is designed as a brief blog to get you thinking about the ways you can prevent pelvic floor tearing during childbirth. Hopefully this will spark an honest discussion with your midwife or OB. As always, knowledge is power! If you want more information, just ask.

What is a perineal tear?
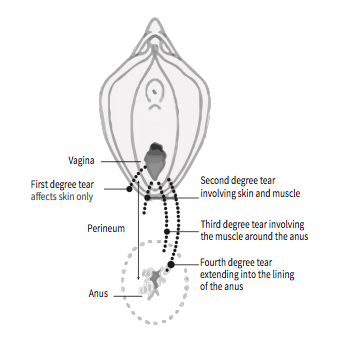
A perineal tear is a tear that affects the skin and muscles of your perineum (the space between your vagina and anus). Tears are rated based on severity, from first degree through to fourth degree.
Many women experience first and second degree tears in vaginal birth, these usually heal without many issues.
Third degree tears extend into the muscles that control your back passage
Fourth degree tears extend into the internal lining of the anus and rectum
Both third and fourth degree tears usually require stitching in an operating theatre and future bladder and bowel function may be compromised in these women.
(stick with me here, I promise there is light at the end of this tunnel)
Approximately 4 out of every 100 women having a vaginal birth experience a 3rd or 4th degree perineal tear
Due to the effects on bowel and bladder control, these women are referred onto Women’s Health physiotherapists for follow up and management. This post will focus on prevention, not treatment. However rest assured, there is treatment available.
There are a few factors that can make you more likely to get a 3rd or 4th degree tear:
if this is your first baby
if you have had a perineal tear in your previous deliveries
you require forceps or vacuum to assist the delivery
if you are of Southeast Asian background
if your baby weighs more than 4kgs
if your baby is posterior (their back against your back)
your babies shoulders become stuck during delivery
So what can be done to help reduce the risk of tearing during childbirth?
WHILST YOU ARE PREGNANT:
Perineal massage
This is done from approximately 35 weeks and can be performed by you or your partner. It can also be assisted with an instrument such as a pelvic wand. Always ask your healthcare provider when is the best time for you to start. It involves strong massage over the perineum to assist in softening and stretching the muscles and soft tissue. (note that it is contraindicated in some pregnancies)
Pelvic Floor Muscle Training
Pelvic floor muscle training in pregnancy has been shown to improve muscle control, and strong flexible muscles may contribute to the optimal descent of your baby’s head during delivery. Carrying out pelvic floor exercises during pregnancy has been reported to protect new mums against a prolonged second stage of labour.
Stretching to encourage optimal baby positioning
There are many stretching and exercise based activities during pregnancy to assist with baby positioning. My favourite positions to teach: forward lean inversions, runners lunge, sumo squat and pelvic tilts (on and off a maternity ball). These movements can assist with moving baby from breech, transverse or posterior into a more ideal position. Head on over to https://spinningbabies.com/ for more info.
Education
Know your own risk, speak with your health professional about any concerns you have and be pelvic floor aware.
DURING LABOUR:
Warm compress
Application of a warm washcloth to your perineum when your baby’s head is crowning to soften the soft tissue and improve stretching ability.
Slow, controlled delivery of baby’s head and shoulders
Consider labour and birthing positions during your second stage that will help your baby to be born slowly, and not pop out in a rush. For example; four point kneeling.
Utilise breathing techniques to assist a slow controlled birth of baby, without direct pushing.
Use hands on technique (midwife, OB or birth support person) to gently support your perineum during the birth of babies head and shoulders
Episiotomy
If you need some extra assistance (with vacuum or forceps) to deliver baby safely, utilise an episiotomy ( a cut made with scissors, at an angle, at the entrance of the vagina). This can reduce the likely of a 3rd or 4th degree perineal tear during use of this equipment.
If I had to leave women with one message on this topic it would be that birth is unpredictable. Yes there are things you can do to reduce your risk as much as possible, but sometimes things will happen during your delivery that mean instruments are the safest option to keep you and your baby safe. A perineal tear does not mean you have failed or that something went wrong. If you have sustained a perineal tear during childbirth, there is LOADS of support out there and lots of great people (like a Women’s Health Physio!) to help support your road to recovery. If you find yourself in this boat a great place to start is www.birthtrauma.org.au
References:
Womens Healthcare Australiasia (WHA) Clinical Excellence Commmission (CEC) Perineal Protection Bundle https://women.wcha.asn.au/collaborative/intervention-bundle
De Leeuw JW, Struijk PC, Vierhout ME, Wallenburg HC. Risk factors for third degree perineal ruptures during delivery. BJOG. 2001;108(4):383–7.
De Leeuw JW, de Wit C, Kuijken JP, Bruinse HW. Mediolateral episiotomy reduces the risk for anal sphincter injury during operative vaginal delivery. BJOG. 2008;115:104–8.
Resar, R., Griffin, F. A., Haraden, C., & Nolan, T. W. (2012). Using care bundles to improve health care quality. IHI innovation series white paper. Cambridge, Massachusetts: Institute for Healthcare Improvement.
Royal College of Obstetricians and Gynaecologists. Third and fourth degree perineal tears, management (Green Top guideline No. 29). London: Royal College of Obstetricians and Gynaecologists; 2015
Van Bavel, J., Hukkelhoven, C.W.P.M., de Vries, C. et al. The effectiveness of mediolateral episiotomy in preventing obstetric anal sphincter injuries during operative vaginal delivery: a ten-year analysis of a national registry. Int Urogynecol J 29, 407–413 (2018)